Introduction
Embryo transfer is often described as the final step of an IVF cycle, yet experienced fertility specialists know it is far more than a routine procedure. A high-quality embryo developed under optimal laboratory conditions can still face reduced implantation potential if the transfer itself becomes technically challenging. For this reason, embryo transfer should be viewed as a critical clinical procedure where preparation, technique, catheter selection, and real-time decision-making all play important roles.
A difficult embryo transfer rarely begins when resistance is first felt during catheter insertion. In many cases, the underlying challenge starts earlier—with patient anatomy, cervical characteristics, previous surgical history, or the choice of transfer catheter. What appears to be a simple resistance at the cervical canal may actually reflect a combination of anatomical and procedural factors that require careful management rather than forceful manipulation.
One of the most common mistakes during embryo transfer is treating every patient as though the procedure will follow the same pathway. In reality, every uterus presents unique anatomical features, and every transfer should be approached with an individualized strategy. Experienced clinicians often spend more time evaluating the patient’s anatomy before the transfer than performing the transfer itself.
Difficult Embryo Transfer Is More Than a Technical Problem
Many publications define difficult embryo transfer simply as resistance during catheter passage. While technically correct, this definition does not fully reflect what clinicians experience in daily IVF practice.
A difficult embryo transfer is not merely the inability to advance a catheter smoothly into the uterine cavity. It is a clinical situation in which anatomical variations, cervical conditions, uterine orientation, or inappropriate device selection require additional interventions that would not normally be necessary during a routine embryo transfer.
These interventions may include:
- Changing the embryo transfer catheter
- Using a guide catheter
- Repositioning the patient
- Modifying the catheter angle under ultrasound guidance
- Performing cervical preparation
- In rare situations, postponing the embryo transfer
Every additional manipulation increases procedure time and may introduce unnecessary cervical or endometrial irritation. Although many difficult embryo transfers still result in successful pregnancies, clinicians generally agree that minimizing trauma and reducing uterine stimulation should always remain the primary objective.
Rather than asking, “How do we complete a difficult transfer?”, experienced IVF specialists often ask a different question:
“How can we prevent the transfer from becoming difficult in the first place?”
That shift in thinking changes the entire clinical approach.
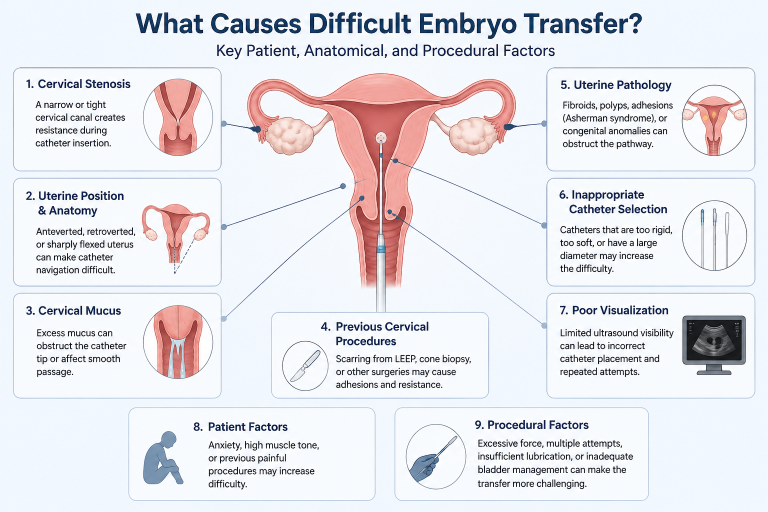
What Causes Difficult Embryo Transfer?
The causes of difficult embryo transfer are rarely limited to a single factor. In most cases, several anatomical and procedural variables interact simultaneously. Understanding these variables before beginning the transfer allows clinicians to make better decisions regarding catheter selection and procedural planning.
1. Cervical Stenosis
Cervical stenosis remains one of the leading causes of technically difficult embryo transfer. A narrowed cervical canal increases resistance during catheter advancement and often tempts inexperienced operators to apply additional force.
However, force should never be considered a solution.
Excessive pressure may cause cervical trauma, bleeding, or uterine contractions—all of which can negatively influence the transfer environment.
Instead, clinicians should first determine why resistance is occurring. Is the narrowing located at the external cervical os? Is there postoperative scarring? Has the patient undergone cervical conization or LEEP? These questions guide the next clinical decision.
In many situations, changing to a catheter that combines a soft atraumatic tip with adequate column strength allows smoother navigation through the cervical canal without excessive bending or buckling. When combined with ultrasound guidance, this approach often reduces the need for repeated catheter insertions.
Importantly, cervical stenosis should not be viewed as an obstacle to overcome through force. It should be considered a signal that the procedural strategy may need to change.
2. Uterine Position and Cervical Alignment
Even when the cervical canal is completely normal, embryo transfer may become difficult because of uterine orientation.
A markedly anteverted uterus, retroverted uterus, or excessive uterine flexion changes the natural relationship between the cervical canal and the uterine cavity. As a result, the catheter may repeatedly contact the anterior or posterior uterine wall instead of following the correct pathway.
Experienced clinicians rarely attempt to solve this problem by increasing insertion pressure. Instead, they modify the transfer angle while observing catheter movement under ultrasound guidance.
This simple adjustment often transforms what initially appears to be a difficult transfer into a smooth and atraumatic procedure.
Pre-procedure ultrasound assessment is therefore valuable not only for measuring uterine depth but also for anticipating catheter trajectory before the transfer even begins
3. Cervical Mucus: A Small Detail with Significant Clinical Impact
Compared with cervical stenosis or uterine anomalies, cervical mucus may appear to be a minor concern during embryo transfer. However, experienced IVF professionals know that even small amounts of excessive mucus can influence the smooth progression of the procedure.
Mucus may adhere to the catheter tip, reduce tactile feedback during insertion, or, in some cases, contribute to embryo retention inside the catheter after transfer. Although the relationship between cervical mucus and pregnancy outcomes remains debated, most IVF centers agree that excessive mucus should be gently removed before embryo transfer.
The key word is gently.
Aggressive cleaning of the cervix may cause bleeding or stimulate uterine contractions, creating a less favorable environment for embryo deposition. The objective is not to achieve a perfectly dry cervical canal but rather to eliminate excess mucus while minimizing cervical manipulation.
This seemingly simple step reflects a broader principle in embryo transfer: every action should reduce, rather than increase, trauma to the reproductive tract.
4. Previous Cervical Procedures and Scar Tissue
A patient’s surgical history often provides valuable clues before embryo transfer begins.
Procedures such as cervical conization, LEEP, repeated cervical dilatation, hysteroscopic interventions, or difficult previous embryo transfers may alter the anatomy of the cervical canal. Scar tissue can create unexpected resistance, false passages, or changes in cervical alignment that are not immediately apparent during routine examination.
This is why reviewing previous treatment records is far more than an administrative task—it is an essential part of procedural planning.
When a difficult transfer is anticipated, the physician can prepare alternative catheter options, adjust the transfer strategy, and ensure ultrasound equipment is available before the procedure starts. Anticipating difficulty is always preferable to reacting to it once the embryo has already been loaded into the catheter.
Why Catheter Selection Matters More Than Many Clinicians Realize
When embryo transfer becomes technically demanding, attention often focuses on the patient’s anatomy. While anatomical factors are important, the characteristics of the transfer catheter itself can substantially influence how the procedure progresses.
An embryo transfer catheter is not simply a tube that carries the embryo. It is a precision instrument designed to balance two competing requirements: flexibility and control.
A catheter that is excessively soft may buckle when resistance is encountered, making advancement difficult. Conversely, a catheter that is overly rigid may increase the risk of cervical or endometrial trauma. The ideal design combines a soft, atraumatic distal tip with sufficient shaft support to allow controlled navigation through the cervical canal.
For this reason, experienced clinicians often evaluate several catheter characteristics before the procedure, including:
- Tip flexibility
- Shaft support (column strength)
- Resistance to kinking
- Smooth trackability through the cervical canal
- Compatibility with ultrasound-guided transfer
- Echogenic visibility of the distal tip
These characteristics become especially important in patients with cervical narrowing, uterine flexion, or previous difficult embryo transfers.
Importantly, no single catheter is ideal for every patient. Instead, catheter selection should be individualized according to anatomical findings and procedural complexity rather than routine preference.
This principle explains why many IVF centers keep more than one embryo transfer catheter available during treatment sessions. Having alternative catheter designs immediately accessible allows clinicians to adapt their strategy without unnecessary delays if unexpected resistance is encountered
Ultrasound Guidance: Turning Observation into Clinical Decision-Making
The introduction of ultrasound-guided embryo transfer has fundamentally changed the way clinicians approach difficult transfers.
Rather than relying solely on tactile sensation, physicians can now observe the movement of the catheter in real time and make immediate adjustments before resistance develops into trauma.
Real-time imaging provides several practical advantages.
First, it confirms that the catheter is following the natural cervical canal rather than creating a false passage.
Second, it helps clinicians recognize whether resistance is caused by cervical anatomy, uterine flexion, or inappropriate catheter orientation.
Finally, ultrasound guidance allows accurate visualization of the catheter tip before embryo deposition, reducing uncertainty during one of the most critical moments of the IVF procedure.
However, ultrasound guidance is only as effective as the visibility of the catheter itself.
As discussed in our previous article, Why Echogenic Embryo Transfer Catheters Are Becoming Essential for Ultrasound-Guided IVF Procedures, echogenic markings significantly improve catheter visualization, allowing clinicians to identify the distal tip more confidently under ultrasound. Improved visibility may reduce unnecessary catheter repositioning and contribute to a smoother transfer, particularly in anatomically challenging cases.
Similarly, successful catheter navigation depends not only on visualization but also on refined transfer technique. In our article Why Embryo Transfer Technique Still Matters in IVF, we explored how careful handling, gentle advancement, and minimizing uterine manipulation remain fundamental principles of successful embryo transfer regardless of catheter design.
Common Mistakes During Difficult Embryo Transfer
1-Applying Excessive Force
One of the most common errors is attempting to overcome resistance by pushing the catheter harder. Although this may occasionally allow catheter advancement, it also increases the risk of cervical trauma, bleeding, and uterine contractions.
When resistance is encountered, clinicians should first determine the underlying cause rather than forcing the catheter forward. Reassessing uterine orientation under ultrasound guidance or selecting a more appropriate catheter is often a safer and more effective solution.
2-Using the Same Catheter for Every Patient
No embryo transfer catheter performs optimally in every clinical scenario. Patient anatomy, cervical characteristics, and uterine position should influence catheter selection.
Experienced IVF specialists often prepare more than one catheter option before beginning the procedure, particularly when previous difficult transfers have been documented.
3-Ignoring Patient History
Previous embryo transfer reports provide valuable clinical information. If resistance, cervical stenosis, or anatomical challenges were encountered during earlier cycles, similar issues may occur again unless procedural planning is modified.
Reviewing previous transfer records before the procedure helps clinicians anticipate challenges and prepare the appropriate equipment.
4-Overlooking Team Communication
Embryo transfer is a coordinated procedure involving both the physician and the embryologist. Clear communication regarding catheter loading, timing, unexpected resistance, or catheter replacement helps maintain procedural efficiency while minimizing the time embryos remain outside the incubator.
Practical Clinical Strategies for Managing Difficult Embryo Transfer
Although every patient presents unique anatomical characteristics, several practical principles can improve the management of technically challenging embryo transfers.
Experienced clinicians commonly recommend:
– Performing ultrasound assessment before embryo transfer.
– Reviewing previous embryo transfer reports.
– Selecting the catheter according to patient anatomy.
– Avoiding repeated catheter insertions whenever possible.
– Maintaining gentle catheter advancement without excessive force.
– Having an alternative catheter available.
– Minimizing cervical manipulation.
– Working closely with the embryology team.
Rather than relying on a single technique, successful difficult embryo transfer usually results from combining careful planning, appropriate device selection, and atraumatic procedural technique.
Does Difficult Embryo Transfer Always Reduce IVF Success?
Although difficult embryo transfer has been associated with lower pregnancy rates in several clinical studies, it should not automatically be considered a predictor of IVF failure.
Implantation depends on multiple factors, including embryo quality, endometrial receptivity, laboratory performance, maternal characteristics, and embryo transfer technique.
Many patients experiencing technically difficult transfers still achieve successful pregnancies when the procedure is carefully managed.
The objective is not simply to complete embryo transfer but to perform it with minimal trauma while maintaining accurate embryo placement inside the uterine cavity.
Conclusion
Difficult embryo transfer should not be viewed as an unexpected complication but as a clinical situation that can often be anticipated and effectively managed.
Understanding the underlying causes—including cervical stenosis, altered uterine anatomy, previous cervical procedures, and catheter-related factors—allows clinicians to adapt their approach before technical challenges arise.
Equally important is recognizing that successful embryo transfer depends on more than operator experience alone. Catheter design, ultrasound visibility, procedural planning, and effective communication between the physician and embryologist all contribute to achieving a smooth, atraumatic transfer.
As IVF techniques continue to evolve, embryo transfer remains a procedure where small technical decisions can make a meaningful difference in clinical practice. Selecting the appropriate catheter for each patient’s anatomy and procedural requirements supports greater procedural confidence while helping create optimal conditions for embryo placement.